For more updates on medicine and advancements in physical therapy, rehabilitative medicine, and health care, visit this blog for Dr. Mary Kneiser.Faced with substantial wariness toward privacy concerns, and continued mocking over fashion concerns, Google Glass is moving away from individual consumers toward a more natural ally of its wearable technology — businesses. More specifically, toward hospitals and doctors who can use Glass as a tool rather than a diversion.
Image Source: thewire.com
A recent study highlighted by Mashable underscored the general problem, as 72 percent of Americans said they won't wear Glass because of privacy concerns. The New York Times puts the conundrum succinctly.
"Consumers have been wary of Glass. Yet it is finding more enthusiastic acceptance in the workplace: in medicine, law enforcement, manufacturing and athletics," The Times writes.
As if on cue, late Monday night Google introduced its Glass at Work program that targets businesses directly. "A number of companies have already teamed up with enterprise software developers to create new ways to serve their customers and to reach their business goals," Google writes. "This is only the beginning of what’s possible for Glass and business." Glass at Work will initially work with the Washington Capitals hockey team, but there are plenty of other areas it can move into easily.
The potential for medicine appears to be the most relevant and dramatic, and several U.S. hospitals have begun equipping doctors with the technology. For example, The Times details a U.C.S.F. lung surgeon who uses Glass during surgery because it shows live images from scans in the corner of his vision while he works. In low-pressure situations, too, like doctor-patient check-ups, some Glass software can hear patient information and automatically input that into electronic medical records. That streamlines the documentation of charts and also allow doctors to spend more time with their patients.
Image Source: thewire.com
Glass even indirectly helped save a life recently, as The Daily Beast highlighted. In an emergency situation where every second mattered, Boston doctors using Glass were able to access a patient's medications and allergies without breaking eye contact. That allowed for quicker help in the high-pressure ER. And given the importance of sterilization in medicine, Glass's voice activation can help doctors access records without needing outside help, or even putting down their instruments.
The strict legal rules of doctor-patient confidentiality and HIPAA regulations also help by making clear what's okay and what's out of bounds privacy-wise. While the public has yet to fully address the legal ramifications of Glass, medicine has clear boundaries. Software for Google Glass used in hospitals have specific protections built in, including keeping information off Google servers and disabling the technology in different locations.
The technology is still in its early phase, of course, but targeting medicine and doctors allows Glass to answer the vexing question of why it needs to exist. “It’s a technology that’s searching for problems to solve, and it’s really a matter of where do the problems emerge?” a chief technologist for business consulting firm PwC told The New York Times. Thus far, those problems point Google to a more corporate-oriented pitch for Glass.
Thursday, April 10, 2014
REPOST: Google Glass Is Finding Its Footing in the Workplace
Far from being merely a spectacles-borne novelty mobile device, Google Glass is finding acceptance in a serious field: modern medicine. Eric Levenson of The Wire writes about the potential held by Google Glass in the emergency room.


Thursday, March 27, 2014
REPOST: Rise of sport science cannot hold back sands of time for footballers
How do medicine and sports science influence a footballer’s form and performance? Sean Ingle of The Guardian investigates.
Image Source: www.theguardian.com
It was a week for football's golden oldies. Samuel Eto'o, at 33, deftly opening the door against Galatasaray and Arsenal and Ryan Giggs, at 40, adding calm and class to Manchester United's engine room against Olympiakos. Arsène Wenger, at 64, chalked up his 1,000th Arsenal game in a daytime "nightmare" at Stamford Bridge.
Amid the eulogies for Wenger, John Hartson spoke of his methods "putting another two or three years" on the careers of Tony Adams, Lee Dixon and Ian Wright. Few would dispute that. In the past decade, those methods have become football's methods. Players are fitter. They recover from training with finely tuned protein-carb shakes, ice baths and massage; not a swift one-two at the pub.
We have come a long way from the days when footballers regarded broccoli as that guy who produced the Bond movies, and only did a downward dog when they slid off a bar stool.
Last year Sir Alex Ferguson said that "sport science is the biggest and most important change in my lifetime". Manchester United monitor 29 variables that may increase a player's susceptibility to injury; sometimes players will be pulled out just before training because something in their data isn't right.
Given such widespread advances, you might expect the average age of players in Europe's top leagues to be climbing sharply. It is not. The Football Observatory recently compared the average age by position of players in the Premier League, Serie A, La Liga, Bundesliga and Ligue 1 from 2005-06 to 2013-14 and found it was also static.
The average age of a first-team defender in the big five European leagues in 2005-06 was 26.21 years; now it is 26.35 – an increase of 0.14 years. The figures for goalkeepers, midfielders and attackers have barely changed either.
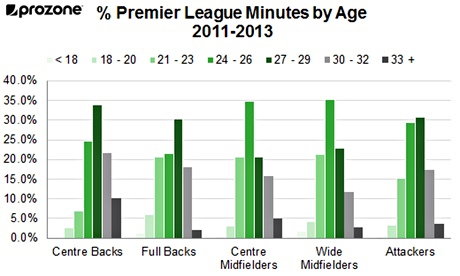
Meanwhile in the Premier League, Prozone's data for the 2011-12 and 2012-13 seasons shows that full-backs 33 or over played just 2.0% of all minutes played by full-backs. For wide midfielders that figure was 2.7%; strikers 3.6% and central midfielders 4.9%. For central defenders – whose positioning can sometimes negate a lack of pace – it was higher at 10.1%.
Image Source: www.theguardian.com
So what is happening? Two things. Sports science is helping older players to stave off the effects of ageing. But, at the same time, the physical demands on footballers is far greater too. So the status quo prevails. Once footballers hit their early thirties they are on borrowed time. Just like they always were.
What is striking, though, is how much faster football has become in the past decade. TV commentators in the 1970s and 1980s were fond of talking about matches being played at 100-miles-an-hour. It was a Sunday morning pootle compared to today's game.
Image Source: www.theguardian.com
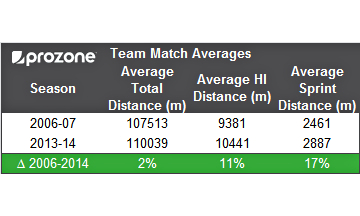
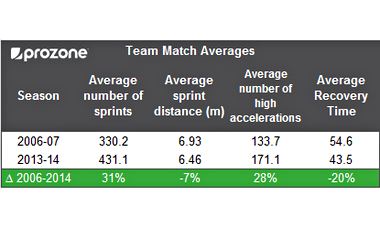
In 2006-07 the average number of sprints per team in a Premier League match was 330.2. This season Prozone's data show that it is 431.1, a 30.6% increase. Meanwhile recovery time between high intensity sprints (speeds of greater than 5.5 metres per second) has dropped from 54.6 seconds to 43.5 seconds, a decline of 20%.

Dr. Mary Kneiser’s nearly 20 years of experience in physical medicine and rehabilitation is decorated with various awards and recognition for her skill and expertise in patient care. Get a glimpse of her highly respected practice by visiting this blog.
Image Source: www.theguardian.com
Perhaps it is not surprising there are so few full-backs, wide midfielders and forwards over 33. They play in positions where a dip in pace is more likely to affect performance. It is not only in road safety adverts where speed kills.
Another development is that clubs monitor GPS and heart-rate data in training. They usually know when a player is 'gone' before we do.
The growth in post- and pre-season tours may also be a factor. Players have less down time to recover in the off-season – so recovery time, which becomes more important with age, can be scarce.
Of course the rate of decline will vary. Genetics, lifestyle, injury history and the number of games can all be a factor. But players are battling against age earlier than is often assumed. Maximal aerobic capacity – or V02 max – peaks around 18 to 20 and while it can plateau until 25 it tends to then decrease by approximately 8-10% per decade.
Dr James Carter, the head of the Gatorade Sport Science Institute at Loughborough University, says that vigorous training after the age of 25 can limit that decline to around 5% per decade but "significant reductions in physiological and performance-related capabilities will be more pronounced once a player enters their thirties".
With some players physiology is not everything. Even in his final season, Paul Scholes's passing figures were as good as ever. Others make themselves relevant in fresh ways. When Giggs still possessed the acceleration of a Maserati and the hips of a ballroom dancer, the ball was lover to nuzzle on those jinking, parabola-like runs; now it is more of a passing acquaintance.
But as a general rule, improvements in sport science and medicine have benefitted younger players as much as older ones. And so veterans are better retained at a similar rate than they were a decade ago. As Carter reminds us, "extending the shelf life of footballers beyond 35, in most cases, is still beyond the remit of science, technology and best practice".
When Giggs and Eto'o started out, football was considered a young man's game. Despite their notable achievements in the past week it still generally is.
Wednesday, February 26, 2014
REPOST: A Woman's Guide To Stroke Prevention
The American Heart Association published a new set of guidelines that focus on preventing stroke in women. The organization highlights the importance of medical history management and early lifestyle changes in stroke prevention. Forbes has the full story below.
A new guideline published in the American Heart Association’s journal Stroke focuses on preventing stroke in the more stroke-prone sex: Women. Though the risk factors for stroke are in large part similar for women and men, women have some additional variables that put them at slightly higher risk throughout their lives. Part of the reason that women are more susceptible than men is simply due to the fact that they live longer. But other factors are largely hormone-related, and relevant to all stages of life.
Stroke is the fifth leading cause of death for men, but for women it’s the third leading cause. Women also tend to have poorer recovery than men, and more residual effects of stroke. They’re also more likely be institutionalized after stroke. Stroke typically occurs when a blood clot forms in a blood vessel going to the brain, thereby depriving it of oxygen.
Changes in the levels of reproductive hormones at different stages of life can affect a woman’s risk of stroke, and this is true for contraceptive hormones at a young age and hormone replacement therapy during menopause. Certain conditions, like preeclampsia, which can significantly raise blood pressure during pregnancy, put a woman at higher risk of stroke both during pregnancy and beyond.
“Women have very unique risks,” said author of the guidelines Cheryl Bushnell, “and they include pregnancy and the complications that can occur with pregnancy, in addition to a high blood pressure during pregnancy, which is preeclampsia and eclampsia. Then there are the issues related to hormonal use such as oral contraceptives and hormones that are used to help treat the symptoms of menopause.”
Here are the major points of the new guidelines:
The take-home message is that prevention should be started earlier than it often is – young women should be thinking about stroke prevention, and talking about it with their doctors. Tracking and managing high blood pressure from an earlier age is the key, according to the authors. So is treating high blood pressure somewhat more aggressively (within reason) during pregnancy.
As always, lifestyle changes are the best ways to reduce the risk of stroke. And these healthy behaviors – eating well, exercising, and not smoking – should be a lifetime endeavor.
“We have a sedentary society, unfortunately,” said Bushnell. “I would emphasis exercise, eating right, and the American Heart Association has the whole Life’s Simple 7. And that’s what I would emphasize for younger women – and all women – who may be at risk for stroke. We’re trying to improve the general health of the population. So all of those actions will help prevent stroke in the future – especially for women.”
Visit this Tumblr blog for Dr. Mary Kneiser for more discussions on physical medicine and rehabilitation.
 |
| (Photo credit: Wikipedia) Image Source: forbes.com |
A new guideline published in the American Heart Association’s journal Stroke focuses on preventing stroke in the more stroke-prone sex: Women. Though the risk factors for stroke are in large part similar for women and men, women have some additional variables that put them at slightly higher risk throughout their lives. Part of the reason that women are more susceptible than men is simply due to the fact that they live longer. But other factors are largely hormone-related, and relevant to all stages of life.
Stroke is the fifth leading cause of death for men, but for women it’s the third leading cause. Women also tend to have poorer recovery than men, and more residual effects of stroke. They’re also more likely be institutionalized after stroke. Stroke typically occurs when a blood clot forms in a blood vessel going to the brain, thereby depriving it of oxygen.
Changes in the levels of reproductive hormones at different stages of life can affect a woman’s risk of stroke, and this is true for contraceptive hormones at a young age and hormone replacement therapy during menopause. Certain conditions, like preeclampsia, which can significantly raise blood pressure during pregnancy, put a woman at higher risk of stroke both during pregnancy and beyond.
“Women have very unique risks,” said author of the guidelines Cheryl Bushnell, “and they include pregnancy and the complications that can occur with pregnancy, in addition to a high blood pressure during pregnancy, which is preeclampsia and eclampsia. Then there are the issues related to hormonal use such as oral contraceptives and hormones that are used to help treat the symptoms of menopause.”
Here are the major points of the new guidelines:
- Women with a history of high blood pressure before pregnancy may be candidates for low-dose aspirin (81 mg) after the first trimester, and/or calcium supplements, to reduce the risk of preeclampsia – dangerously high blood pressure during pregnancy.
- Preeclampsia confers twice the risk of stroke and four times higher risk of high blood pressure later in life. Its stroke risks last well after pregnancy, so doctors should consider it a risk factor just like the classic ones: Cholesterol, smoking, and obesity.
- Doctors should consider treating pregnant women with moderately high blood pressure (150-159 mmHg/100-109 mmHg) with medication. Pregnant women with severely high blood pressure (160/110 mmHg or above) should generally be treated (some medications are not safe during pregnancy, however).
- Before starting birth control pills, women should be screened for high blood pressure, since the hormones in birth control can increase the risk of stroke.
- Women who have migraines with aura should stop smoking to avoid higher stroke risks. Migraine headaches that are accompanied by aura have been linked to increased stroke risk.
- Women over the age of 75 should be screened for atrial fibrillation, as it is associated with higher stroke risk.
- Hormone therapy during menopause may increase the risk of stroke, although the data are conflicting. But hormone therapy should not be used to prevent stroke.
- Psychosocial stress and depression are more common in women than in men, and are associated with significantly higher risk of stroke.
The take-home message is that prevention should be started earlier than it often is – young women should be thinking about stroke prevention, and talking about it with their doctors. Tracking and managing high blood pressure from an earlier age is the key, according to the authors. So is treating high blood pressure somewhat more aggressively (within reason) during pregnancy.
As always, lifestyle changes are the best ways to reduce the risk of stroke. And these healthy behaviors – eating well, exercising, and not smoking – should be a lifetime endeavor.
“We have a sedentary society, unfortunately,” said Bushnell. “I would emphasis exercise, eating right, and the American Heart Association has the whole Life’s Simple 7. And that’s what I would emphasize for younger women – and all women – who may be at risk for stroke. We’re trying to improve the general health of the population. So all of those actions will help prevent stroke in the future – especially for women.”
Visit this Tumblr blog for Dr. Mary Kneiser for more discussions on physical medicine and rehabilitation.
Wednesday, January 15, 2014
REPOST: For young athletes, injuries need special care
Sports medicine is a need for athletes of all ages to help their bodies heal from injuries quickly and get back to top form. Laura Landro of the Wall Street Journal writes about the growing need for physical medicine departments of pediatric hospitals to accommodate teen and preteen athletes.
Children's hospitals are expanding programs to care for a fast-growing category of young patients: injured athletes.
The rehabilitation needs of children and teens are different than those of adults. More sports medicine programs are working exclusively with young athletes, using surgical techniques and physical therapy protocols that don't interfere with growing bones and cartilage.
One aim of this is to prevent affecting the growth plate—the area of growing tissue near the end of long bones in children and teens. For example, while adults may lift heavier weights to build muscle during physical therapy, pediatric patients may do higher repetitions with lower resistance to avoid hurting growing bones, muscles and tendons. The programs also offer encouragement and support for kids upset to be sitting out of a beloved sport.
More than 3.5 million children a year receive treatment for sports injury, according to Stop Sports Injuries, a campaign whose backers include the American Orthopaedic Society for Sports Medicine. And high-school athletes account for an estimated 2 million sports injuries each year. While concussions account for about 15% of youth sports injuries, experts say many sports carry risks for musculoskeletal injuries, in large part due to increased emphasis on year-round competition, single-sport concentration and intense training regimens.
A study published last year by Boston Children's Hospital warned that children of all ages are sustaining significant sports injuries that require surgical intervention. "In the past we'd put a cast on a broken leg, take it off six to 13 weeks later and send kids home," says Lyle Micheli, director of the hospital's division of sports medicine. "Now we realize we have to very systematically rehabilitate these kids for strength and basic function, and determine when it is safe for them to return to play."
While injuries from recreational activities such as biking have fallen over the last decade, team sports including football and soccer saw injuries rise by 22.8% and 10.8% respectively, according to a study last year by Cincinnati Children's Hospital Medical Center.
Doctors are seeing more overuse injuries. There has been a fivefold increase since 2000 in the number of shoulder and elbow injuries among youth baseball and softball players, according to Stop Sports Injuries.
Children's Hospital & Research Center Oakland, in California, last fall opened a Sports Medicine Center for Young Athletes at its Walnut Creek campus. "It's hard for kids to do rehabilitation next to an 85-year-old stroke victim or a 75-year-old cancer patient," says Nirav Pandya, the center's director, and an orthopedic surgeon. The center and many other pediatric clinics offer classes and programs to help kids improve sports performance while avoiding injury.
Physical therapy after injury and surgery, such as repair to the anterior cruciate ligament in the knee, is covered by insurance for varying periods. After that, clinics may design a regimen children can perform at home or at a local fitness facility.
Jeremy Frank, a pediatric orthopedic surgeon at Memorial Healthcare System's Joe DiMaggio Children's Hospital in Hollywood, Fla., says that there is often little pain a week after minimally invasive ACL surgery, so young people "think they are good to go and don't realize they have six months of rehabilitation in front of them." Often, he says, there is a "bargaining moment" where his young patients try to get him to approve more activity than they are ready for. Patients are generally referred to Memorial's two U-18—for Under 18—physical rehabilitation clinics in Coral Springs, Fla., where therapists work with families and coaches to stress the importance of healing.
Dr. Frank, U-18's assistant director, says while the vast majority of athletes get back to sports and do well, there are times when a young patient sustains multiple injuries such as a third ACL tear. "You have arthritic changes in your knee, and you have to stop playing soccer," he says.
Dylan Rupert, 17, a running back and captain of the Cypress Bay High School football team in Weston, Fla., tore his ACL during play last fall. His parents opted for a repair technique, which surgeons are more often using in pediatric patients. The procedure avoids drilling through the growth plate and may decrease risks of future pain and re-injury. The surgery used part of Dylan's own hamstring rather than a cadaver tissue more commonly used in adults. He started rehab at Coral Springs three days after his Oct. 22 surgery.
The injury was devastating for Dylan. It came just as he was getting the attention of college coaches, says his mother, Monica Puga-Finch, an information technology program director at the clinic's parent Memorial. In his first physical therapy session, senior therapist Whitney Chambers helped calm his fears, but "told him that she was going to push him, and he couldn't say 'I can't.' " As the sessions continued twice a week he would often come out sweating and sore but excited, "with a sense of accomplishment," Ms. Puga-Finch says. Ms. Chambers helped with the emotional aspects of being sidelined, encouraging him to go to practices and games with his team. His rehabilitation is expected to take six to eight months. He plans to return to sports in college.
Ms. Chambers says physical therapy after the growth-plate sparing procedure is more conservative than for the traditional ACL reconstruction. It starts with protective weight bearing exercises using crutches and a knee brace, gentle range of motion work, and ice and electrical stimulation for swelling and pain control. Then she works on strengthening muscles and restoring joint flexibility. To make it more fun, she uses games or obstacle courses.
The clinic uses screening questionnaires to identify kids at risk of depression, who may be referred to a child psychologist.
Kaylyn Lambertt who has played soccer from the age of 6, was a junior in high school when she felt a searing pain in her left hip during a game in December 2010. She continued to play for months as it got worse. Her labrum, part of her hip joint, was torn in two places, with a socket out of place. A lump on her bone was wearing down the cartilage every time she walked or ran. She had surgery to repair the damage in 2011, followed by months of rehabilitation with Ms. Chambers.
She returned to soccer her senior year, but began feeling pain, this time in her right hip. Dr. Frank told her that she had torn the labrum. She underwent a second surgery in December 2012. She returned to Ms. Chambers and realized during their talks that "soccer isn't everything." Now a freshman at Florida State University she plays a pickup game of soccer now and then, but is focused on what Ms. Chambers inspired her to chose as a career: physical therapy.
Dr. Mary Kneiser has behind her two decades worth of experience as a physical medicine and rehabilitation specialist. Visit this Facebook page for more updates.
Children's hospitals are expanding programs to care for a fast-growing category of young patients: injured athletes.
 |
| Kaylyn Lambertt, a high-school soccer player and now a freshman at Florida State University, had surgery on her left hip her junior year and her right hip her senior year. Image source: wsj.com |
The rehabilitation needs of children and teens are different than those of adults. More sports medicine programs are working exclusively with young athletes, using surgical techniques and physical therapy protocols that don't interfere with growing bones and cartilage.
One aim of this is to prevent affecting the growth plate—the area of growing tissue near the end of long bones in children and teens. For example, while adults may lift heavier weights to build muscle during physical therapy, pediatric patients may do higher repetitions with lower resistance to avoid hurting growing bones, muscles and tendons. The programs also offer encouragement and support for kids upset to be sitting out of a beloved sport.
More than 3.5 million children a year receive treatment for sports injury, according to Stop Sports Injuries, a campaign whose backers include the American Orthopaedic Society for Sports Medicine. And high-school athletes account for an estimated 2 million sports injuries each year. While concussions account for about 15% of youth sports injuries, experts say many sports carry risks for musculoskeletal injuries, in large part due to increased emphasis on year-round competition, single-sport concentration and intense training regimens.
A study published last year by Boston Children's Hospital warned that children of all ages are sustaining significant sports injuries that require surgical intervention. "In the past we'd put a cast on a broken leg, take it off six to 13 weeks later and send kids home," says Lyle Micheli, director of the hospital's division of sports medicine. "Now we realize we have to very systematically rehabilitate these kids for strength and basic function, and determine when it is safe for them to return to play."
 |
| Image source: wsj.com |
While injuries from recreational activities such as biking have fallen over the last decade, team sports including football and soccer saw injuries rise by 22.8% and 10.8% respectively, according to a study last year by Cincinnati Children's Hospital Medical Center.
Doctors are seeing more overuse injuries. There has been a fivefold increase since 2000 in the number of shoulder and elbow injuries among youth baseball and softball players, according to Stop Sports Injuries.
Children's Hospital & Research Center Oakland, in California, last fall opened a Sports Medicine Center for Young Athletes at its Walnut Creek campus. "It's hard for kids to do rehabilitation next to an 85-year-old stroke victim or a 75-year-old cancer patient," says Nirav Pandya, the center's director, and an orthopedic surgeon. The center and many other pediatric clinics offer classes and programs to help kids improve sports performance while avoiding injury.
Physical therapy after injury and surgery, such as repair to the anterior cruciate ligament in the knee, is covered by insurance for varying periods. After that, clinics may design a regimen children can perform at home or at a local fitness facility.
Jeremy Frank, a pediatric orthopedic surgeon at Memorial Healthcare System's Joe DiMaggio Children's Hospital in Hollywood, Fla., says that there is often little pain a week after minimally invasive ACL surgery, so young people "think they are good to go and don't realize they have six months of rehabilitation in front of them." Often, he says, there is a "bargaining moment" where his young patients try to get him to approve more activity than they are ready for. Patients are generally referred to Memorial's two U-18—for Under 18—physical rehabilitation clinics in Coral Springs, Fla., where therapists work with families and coaches to stress the importance of healing.
Dr. Frank, U-18's assistant director, says while the vast majority of athletes get back to sports and do well, there are times when a young patient sustains multiple injuries such as a third ACL tear. "You have arthritic changes in your knee, and you have to stop playing soccer," he says.
Dylan Rupert, 17, a running back and captain of the Cypress Bay High School football team in Weston, Fla., tore his ACL during play last fall. His parents opted for a repair technique, which surgeons are more often using in pediatric patients. The procedure avoids drilling through the growth plate and may decrease risks of future pain and re-injury. The surgery used part of Dylan's own hamstring rather than a cadaver tissue more commonly used in adults. He started rehab at Coral Springs three days after his Oct. 22 surgery.
The injury was devastating for Dylan. It came just as he was getting the attention of college coaches, says his mother, Monica Puga-Finch, an information technology program director at the clinic's parent Memorial. In his first physical therapy session, senior therapist Whitney Chambers helped calm his fears, but "told him that she was going to push him, and he couldn't say 'I can't.' " As the sessions continued twice a week he would often come out sweating and sore but excited, "with a sense of accomplishment," Ms. Puga-Finch says. Ms. Chambers helped with the emotional aspects of being sidelined, encouraging him to go to practices and games with his team. His rehabilitation is expected to take six to eight months. He plans to return to sports in college.
Ms. Chambers says physical therapy after the growth-plate sparing procedure is more conservative than for the traditional ACL reconstruction. It starts with protective weight bearing exercises using crutches and a knee brace, gentle range of motion work, and ice and electrical stimulation for swelling and pain control. Then she works on strengthening muscles and restoring joint flexibility. To make it more fun, she uses games or obstacle courses.
The clinic uses screening questionnaires to identify kids at risk of depression, who may be referred to a child psychologist.
Kaylyn Lambertt who has played soccer from the age of 6, was a junior in high school when she felt a searing pain in her left hip during a game in December 2010. She continued to play for months as it got worse. Her labrum, part of her hip joint, was torn in two places, with a socket out of place. A lump on her bone was wearing down the cartilage every time she walked or ran. She had surgery to repair the damage in 2011, followed by months of rehabilitation with Ms. Chambers.
She returned to soccer her senior year, but began feeling pain, this time in her right hip. Dr. Frank told her that she had torn the labrum. She underwent a second surgery in December 2012. She returned to Ms. Chambers and realized during their talks that "soccer isn't everything." Now a freshman at Florida State University she plays a pickup game of soccer now and then, but is focused on what Ms. Chambers inspired her to chose as a career: physical therapy.
Dr. Mary Kneiser has behind her two decades worth of experience as a physical medicine and rehabilitation specialist. Visit this Facebook page for more updates.
Subscribe to:
Posts (Atom)